
Tables are best viewed in landscape mode on mobile devices
Table 1
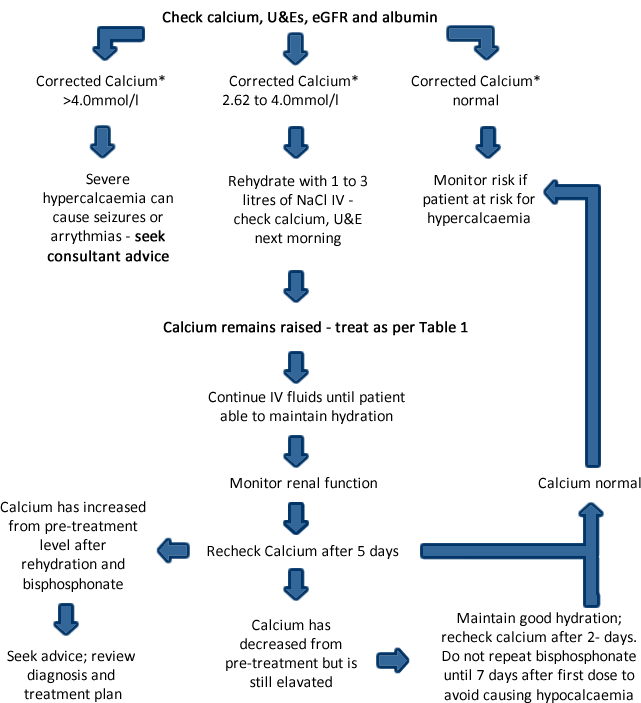
| Corrected calcium* (mmol/l) | Drug and Dose | Diluent and maximum infusion rate |
| Disodium pamidronate | ||
| 2.62 to 3.0 | 15mg to 30mg | 500ml NaCl 0.9% over > 60 minutes |
| 3.0 to 3.5 | 60mg | 500ml NaCl 0.9% over > 60 minutes |
| 3.5 to 4.0 | 90mg | 500ml NaCl 0.9% over > 90 minutes |
| >4.0 | 90mg | 500ml NaCl 0.9% over > 90 minutes |
| Zoledronic acid | ||
| >3.00 | 4mg | 100ml NaCl 0.9% over 15 minutes |
If corrected calcium >3.0mmol/l, some units routinely give pamidronate 90mg as a higher dose.
*Corrected calcium = Measured calcium +0.022 x (40 - serum albumin g/l)